
ARTICLE SUMMARY:
Leaders from Hologic, Siemens Healthineers and DeepLook Medical discuss how medtech can help improve women’s health outcomes with innovative diagnostic tools and a focus on investment and inclusivity. By Camille Emma Schilkie and Terri Petmezas, ZS.

ZS
ZS intimately understands the complexities of the medtech market, and we can help you connect the dots across your organization, from strategy through commercialization.
Across medtech and healthcare more broadly, we have the opportunity to help address diagnostic and treatment disparities that affect women.This long-standing problem not only represents a moral imperative, but it also presents business opportunities for those willing and able to act. Innovative diagnostic tools and treatment solutions are essential for improving women’s health outcomes. Yet current investment in this area falls short, as there’s only approximately 2% of medtech funding devoted to non-cancer-related women’s conditions.
As part of our Women in Medtech group, ZS hosted a panel discussion on how increased research, development and funding in women’s health is paramount. The panel included: Jennifer Schneiders, president of diagnostic solutions at Hologic; Amanda DePalma, SVP, head of corporate and regional marketing, ultrasound at Siemens Healthineers; Marissa Fayer, CEO of DeepLook Medical and HERhealthEQ. Camille Emma Schilkie and Terri Petmezas, both associate principals in ZS’s medtech practice and leaders of ZS’s Women’s Health Expertise Hub for Medtech, moderated the discussion.
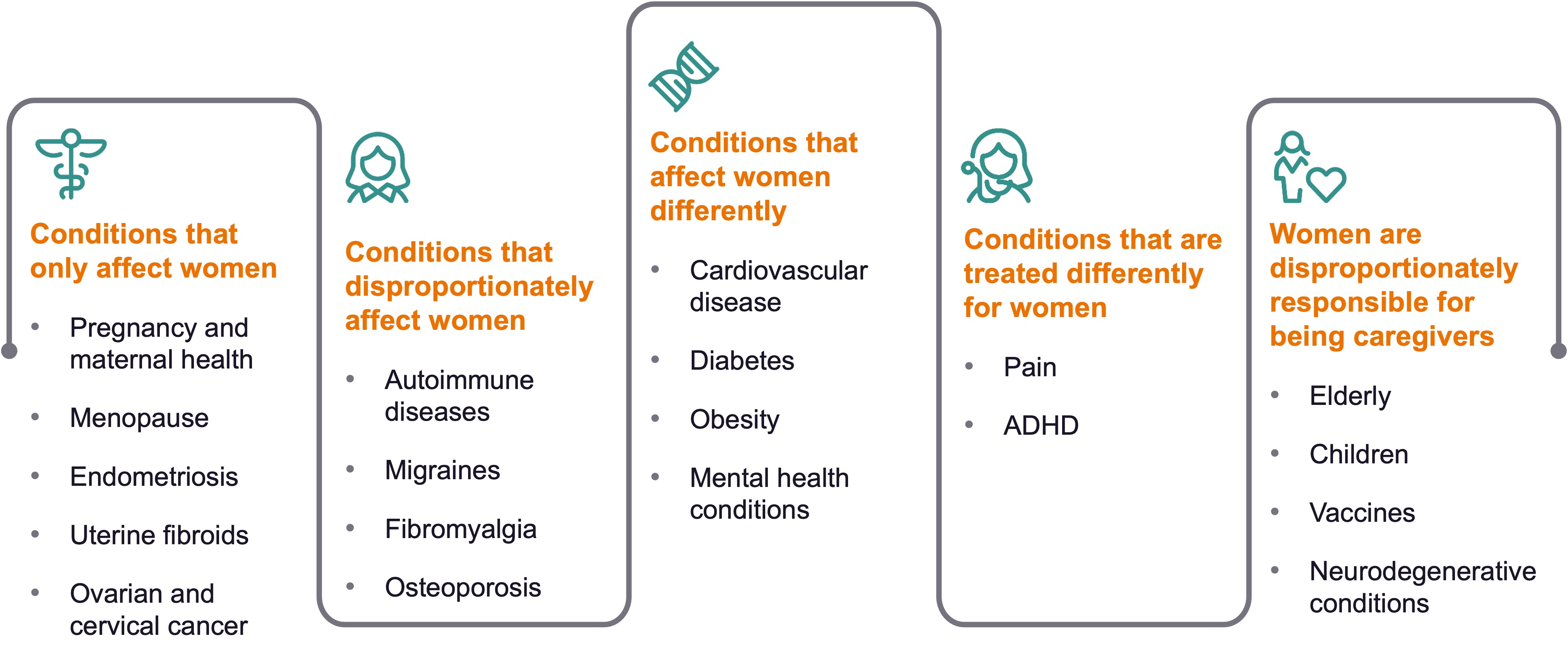
The discussion started with the definition of women’s health, which extends beyond reproductive health. It encompasses conditions that solely affect women such as menopause, endometriosis, cervical cancer and ovarian cancer. But it also includes conditions that disproportionately affect women such as autoimmune diseases and migraines, as well as those that affect all genders but present differently in women such as cardiovascular disease and diabetes.
The conversation highlighted significant gaps in research and investment in women’s health. For instance, ovarian and cervical cancers are highly lethal but receive limited funding. Many women experience delays in diagnosis for conditions such as endometriosis, often taking up to 10 years. The panelists further explored these issues and the need for increased attention and resources in women's health.
Camille Emma Schilkie: What’s your perspective on diagnostic and treatment issues that solely, differently and disproportionately affect women?
Jennifer Schneiders: It always surprises me how much we take for granted. We often don’t realize the gaps that exist in traditional women’s health issues, such as breast cancer and cervical cancer, and also outside of those more well-known conditions. One thing that’s important here is educating the industry about clinical trials and how we think about research. How do we incorporate more diversity in trials and then continue to fund and promote inclusion? Then it’s taking some baby steps to close the gaps. You can’t make all these changes at once and expect things to immediately get better.
Marissa Fayer: When we think about breast cancer and heart disease, for example, we need to think about how they affect families and communities. What technology and tools need to be tailored for women and for different communities of women? How are we making sure they have access?
Amanda DePalma: There has been increased attention on women’s health lately, especially looking outside of reproductive care. This is great, but it’s not yet enough. The White House Initiative on Women’s Health Research intends to create an additional $12 billion of investment in research specific to women’s health issues. How do we get from conversation to action and create enough focus to drive real change? I think we saw during the pandemic that we can move fast if we want to, but it requires everyone to come together to make decisions and move forward. How can women benefit now from improved outcomes and not have to wait for them to come years from now?
Schneiders: The focus of our business is not a trade-off. We don’t want to take away from the progress we’ve made in areas such as breast cancer screening. This is not an “or” but rather an “and” to make progress in underserved and underinvested areas of women’s health.
Fayer: I also want to say we’re not taking away from men’s health.
FIGURE 1: Understanding Women’s Unique Healthcare Disparities, Differences and Ecosystem Roles
Terri Petmezas: Well said—it’s not a zero-sum game. What is medtech’s responsibility to address disparities in terms of helping with diagnostics challenges andgettingpatients to the appropriate treatment faster?
DePalma: We have to ensure diversity in clinical trials. It’s good to see that there are now diversity requirements in many countries. That said, we need to not only design the trials to require diversity but also get out into communities and bring in the right participants. How do we build trust? How do we provide resources such as ride sharing to get people to a study to enroll and also be there for the follow-up? This will be important so we can track conditions to understand how innovations affect outcomes.
Fayer: It’s our responsibility in medtech to drive the change and innovation and do the work. The areas have been identified. We have to put in the money, the resources, the time and the effort.
Schneiders: The reality we face depends on the size of the company, whether it’s publicly traded and the strengths of that company. I often see that a startup is able to garner funding that can fuel a new technology or innovation. Then the publicly traded company can acquire that asset andusecommercial resources to promote it, get reimbursement and provide all the things needed to fuel the business. Therefore, it’s really important for companies to work together, collaborate or partner in this field.
DePalma: That’s right. The ecosystem we work in is really important to maintain. Big, revolutionary innovation can get lost in large companies. We have lots of processes, lots of business cases. Startup companies can be bold and nimble, but they need funding. How do we keep that ecosystem going? Oftentimes some of these startups are founded by clinicians that see a problem they’re dealing with every day—something that might seem very simple—so they innovate around it, and then it fits perfectly into the portfolio of a larger company. It’s really important that we keep the ecosystem whole to drive innovation to meet patient and customer needs.
Petmezas: I’m curious about your reflections on collaboration and how you see it playing out with medtech, pharma, government, nonprofits and patient advocacy groups, given that no one entity is able to tackle this alone.
Fayer: We have to do the work together, we have to be in the same room and we need to talk about it. Women control 80% to 85% of healthcare spend and are 51% of the population. The world is better when we are healthy. It’s everybody working together in collaboration to get there, including small companies, large companies, payors and legislators. And let’s be realistic. One entity can’t get us there to drive the innovation needed. We need work together, and the barriers need to be broken down.
DePalma: I see a few mechanisms that can facilitate collaboration. AdvaMed, a medtech industry association,does a great job pulling the industry together at times when we may typically compete. It brings us together to tackle the big problems. There are a lot of forums,such as Medtech Innovator, that focus on diverse innovators. There’s so much work to do that connecting these dots will help us all, especially patients and clinicians.
Schilkie: How do we drive investment into women’s health? How do we make sure that the right decision-makers are in the room?
Schneiders: At Hologic, we’ve invested in the Hologic Global Women’s Health Index. This survey looks at various aspects of women’s health outside traditional measures and includes data from roughly 147,000 women across the globe. It’s helping us target key areas in women’s health where we believe we can collectively make a difference and invest. We cannot solve all issues at once. We need collaboration among different organizations to overcome complexities and bring innovations to fruition. Sometimes I think organizations invest in things without fully appreciating what they will take to get across the finish line. Without that appreciation, it’s hard tobalance thescope of improvement we can expect if we are successful. That said, the first step is investing in data and information that helps us target the key areas of focus, which is critically important.
DePalma: What we’ve done at Siemens Healthineers is focus on access to care. What can we do with our own portfolio organically? What can we do with investments with strategic partners that help us provide access to care to underserved or underrepresented populations, in both developed and developing markets? For example, we’ve partnered with one of our distributors to build an ultrasound manufacturing facility in Ethiopia. Not only does that make ultrasound systems available in Ethiopia, but it also creates jobs. It creates that ecosystem we talk about needing. It enables access and the ability to get to care.
One thing we can all do independently is look at angel investing. The innovation that is out there pre-seed is fascinating. You can focus on female founders and Black founders in medtech or any industry. It doesn’t take a lot of money. And you can pool your money with other investors and put your money where your mouth is. Even small investments can make a difference.
Fayer: At a time when women have more control over money and are making more money, we can move money into women’s health companies or into companies that are run by women. A full 85% of women’s health companies have either a woman founder or cofounder. Invest in women. You can start out as low as a few thousand dollars. Also, many of these women’s health companies are going direct to consumer, and we can support them by purchasing their products.
I also encourage nonmonetary support of women’s health companies such as making introductions or providing mentorship. Women CEOs and founders in smaller companies need the support of women in larger corporate roles. For ZS, maybe there is a consulting opportunity or a role you can play in connecting people and driving collaboration, as we’ve discussed.
Petmezas: How do we think portfolio strategies need to evolve to be more inclusive of women? For example, in pharmaceuticals, we now have treatments for rheumatoid arthritis that include pregnant women. How can we be more inclusive of women’s needs?
Fayer: Inclusive portfolios mean we all need to invest in technologies and innovation that address the disparities in women’s health. As an early-stage investor at an early-stage company, I see so many different ideas and reports that highlight the disparities. Take any one of these ideas. Incubators, accelerators, investors and larger companies should support these ideas, which are creative and foster technologies that fill gaps.
The other part is ensuring inclusivity in clinical trials. One thing we did at Deeplook was enforce this. We know that dense breast tissue disproportionately affects Black, Asian and Jewish women. Therefore, we wrote into the protocol that there must be 40% Black women, 20% Asian women and so on, included in the study. Diversity in trials needs to be an imperative. Foster innovation that specifically addresses disparities.
Schneiders: I think it’s incumbent upon us to take advantage of the data that’s coming out. Don’t just read it and put it aside. All of us working in this industry have to be bold. We have to have a voice at the table and use our voice to speak to the data and educate ourselves and others on the data so we can stand up for women’s health.
Schilkie: Some studies find that conditions solely affecting women are reimbursed at a lower rate. How do we use our data to educate payors and make sure diagnostics and treatments are properly reimbursed?
Schneiders: Within our surgical division, we looked at a publication that outlined how gynecological surgical procedures are reimbursed for significantly less, if you equate them to similar procedures for men. While this is a huge issue, there’s an even larger issue due to the potential downstream effects. In the article, they call this double discrimination.There is the potential that surgery students may not want to go into gynecological surgery due to the lower reimbursement and pay. Therefore, there may be a negative effect on talent and the number of people who go into the field.
This publication helped to create awareness. It made me think, “How did we get to this point? Who is standing up and advocating?” At Hologic, we have resources associated with market access, reimbursement and payors. This is an opportunity for us, with our voice and within the forums we have, to speak to key stakeholders, educate them and uncover opportunities to influence a different direction to ensure reimbursement is where it needs to be as compared to the standard for other procedures.
DePalma: Reimbursement must be considered early when you’re developing solutions and innovations. If a solution will not be paid for, it will not get adopted, and that includes both the facility fee as well as the physician fee. The process is complex and requires significant effort, especially for new or more expensive procedures that offer better outcomes You’ve got to engage your thought leaders in your clinician community to advocate with the Centers for Medicare & Medicaid Services. You’ve got to get them coding procedures, even if they’re not yet getting paid. This is a big education opportunity. We must help people as they’re thinking about innovations and commercialization plans to make sure they understand the steps, and also the consequences, of reimbursement.
Schneiders: We also don’t want to negatively affect reimbursement that’s been set for other procedures. It’s not a give and take. It’s an “and,” not an “or.”
Fayer: You also have to consider reimbursement when you’re going through regulatory procedures. Maybe it’s a breakthrough designation that puts you on the top of the list for Current Procedural Terminology (CPT) code review and potential acceptance. There are a lot of CPT codes out there. Maybe they just need to be translated differently. You have to think about this because a hospital or doctor can’t order tests and procedures without being reimbursed.
Petmezas: How do you think about partnering with healthcare providers (HCP) to improve care pathways and protocols to close gaps in women’s health?
DePalma: You have to have a clear understanding of your stakeholders who are making decisions around care pathways and protocols. What are the improved outcomes that are going to be delivered, both clinically and economically? You’ve got to be able to articulate that. You may not always have a big clinical study, but if you have a pilot, you can demonstrate feasibility. If you understand the problems your customers face and the care pathways and solutions they’re using, you can help streamline them. You can quantify potential results. I think you have to speak their language, understand their needs and demonstrate you’re going to do what you say you can do.
FIGURE 2: Connecting the Dots to Drive Innovation and Investment in Women’s Health
Fayer: With small companies, it’s really hard to get to physician adoption, so start small with smaller hospitals and clinics that don’t have a very large Institutional Review Board process and private practices. Then start to scale up, maybe with individual HCPs. Think about creative ways to get clinician feedback because your innovation will not move forward without it. Then maybe it’s a partnership with a large corporation to use its relationships at bigger clinician feedback centers. Let’s get our innovations to patients quickly and then iterate at the same time. Start small and then grow.
Schilkie: To wrap up, what is one piece of advice that you would give to a strategic partner like ZS to make an impact in these important areas?
Schneiders: No one can solve all of these problems. My advice is to continue to educate yourselves and others on these important issues, and then focus on the key areas where you can build strong expertise or where you feel you can drive change through your partnerships and collaborations. Prioritize areas where you think you can have the greatest impact.
DePalma: The reason the industry works with consultants is because we can tap into the broad industry perspective you have and your visibility into what best practices look like. ZS is a trusted partner, so continue to bring your insights and challenge the status quo. Let’s work together to have real conversations that can turn to action.
Fayer: Be the change. Ask for it. Challenge what you see happening if it’s not going to drive the progress that you think we need. Also, show us that these issues are important to you. Show how you’re investing in women and making sure enough women have a seat at the table. How are the men in your organization showing up as allies, advocating for the women they work with? If we want to make meaningful change in this industry, we all need to work together.

 Camille Emma Schilkie and Terri Petmezas are both Associate Principals at ZS.
Camille Emma Schilkie and Terri Petmezas are both Associate Principals at ZS.
ZS is a management consulting and technology firm that partners with companies to improve life and how we live it. We transform ideas into impact by bringing together data, science, technology and human ingenuity to deliver better outcomes for all. Founded in 1983, ZS has more than 13,000 employees in over 35 offices worldwide. To learn more, visit www.zs.com or follow us on LinkedIn
Learn more at ZS